- Visibility 56 Views
- Downloads 7 Downloads
- DOI 10.18231/j.ijmi.2022.022
-
CrossMark

A proposed new classification of maxillary sinus using panoramic radiograph
- Author Details:
-
 Joseph Johny *
Joseph Johny *
-
Timy S Alex
-
Athulya B Mohan
Introduction
Maxillary sinus is the first paranasal sinus to develop located in the body of maxilla which is also known as “Antrum of Highmore".[1] It develops at 17th week of the prenatal period. 50% of its final size is reached by the end of 8th year and maximal values of all diameter and volume are reached by the end of 16th year.[2] They exhibits significant inter individual and intraindividual variation[3]
Lerno classified shapes of maxillary sinus into triangular, oval, curved, rectangular and square shapes[4] while shapes of its base were classified into triangular, leaf, scapular and renal shape.[5] 17% sinus asymmetry and 83% symmetry were noted in a study by Maryam et al.[6]
Studies states that maxillary septa, which are the bony cortical structures traversing the maxillary antrum, appeared to have a relation with tooth development.[7] Underwood[8] in 1910 first described it in detailed anatomy of the maxillary sinus; thus it is referred to as Underwood’s septa. Underwood[9] establish that septa arises from the area between two adjacent teeth whereas, Neiver [10] proposed that the embryonic out-pouching of the ethmoidal infundibulum producing fingerlike projections derives septa. Sinus septa had been classified into primary (septa that occur along the development of maxilla) and secondary (septa that occur as a result of irregular pneumatization of the sinus floor after tooth loss) by Krenmair.[11] Most common complication with the septa is the risk of Schneiderian membrane perforation during sinus operations.[12], [13], [14] Therefore a detailed study of sinuses are of importance during dental implantation and sinus lift procedures.[15] Septae gives rise to multiple recesses.[8]
The relation of sinus contour and sinus floor elevation surgery was first described by Niu et al. They classified sinus with recess into Buccal recess and Palate-nasal-recess(PNR).[16] Angle A which is the angle between buccal and palatal alveolar walls shown by Cho et al. is related increased risk for perforation.[17] Sharper angles at premolar region also poses increased risk for membrane perforation as suggested by Velloso et al.[18] The intersection point of two imaginary lines following the lower part of the lateral nasal wall and the palatal wall in the maxillary sinus is described first as Palate-nasal-recess(PNR) by Wang et al.[19]
As an important anatomical structure the maxillary sinus is a subject of various interventions in rhinological endoscopic, ophthalmic and maxillofacial surgery and neurosurgery. The main aim of maxillary sinus operations is to preserve its anatomical and functional integrity. This is possible after preoperative assessment of the morphological characteristics of the sinus such as its volume, linear dimensions, wall thickness, septa, position and permeability of its drainage ostium.[20]
Dtailed research and modern clinical interpretation of the anatomy, physiology and pathology of the maxillary sinus are an important condition for the development and improvement of modern operative and reconstructive techniques and for the prevention of postoperative complications.[20]
Subjects and Methods
A total of 1000 digital panoramic radiographs available in computer as softcopies in the Department of Oral Radiology in Sree Anjaneya Institute of Dental Sciences were selected for this study. The radiographs having positional and magnification errors were excluded during selection process. The panoramic radiographs were taken with KODAK 8000 carestream machine with exposure parameters 73kVp, 12mA, 13.9 seconds. The selected radiographs included 18-50 years of age group. The collected data was entered in spreadsheet and was analysed statistically. The criteria for selection includes (1) Patients between 18 to 50 years were included (2) Both dentate and partially dentate patients were included (3) Edentulous patients were excluded (4) Radiographs with positional and magnification errors were excluded. Protocol number of ethical committee-SAIDS/IHEC/21/202.
Results
Classification by shape
A total of 1000 softcopies of panoramic radiographs were taken from hard drive of Oral Radiology Department in Sree Anjaneya Institute of Dental Sciences.
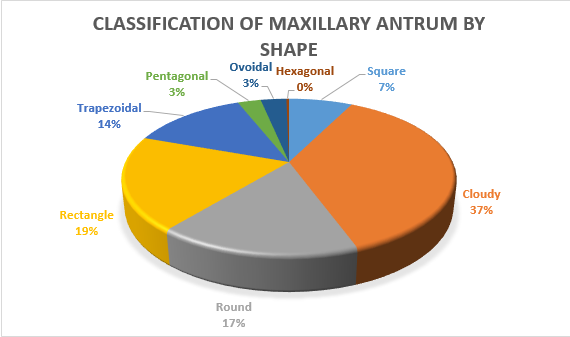
The contour of medial wall, posterior wall, floor and an imaginary line connecting the superior points of medial and posterior walls were outlined. Among 2000 maxillary antrums we observed 8 shapes by outlining the contour of medial wall, posterior wall,
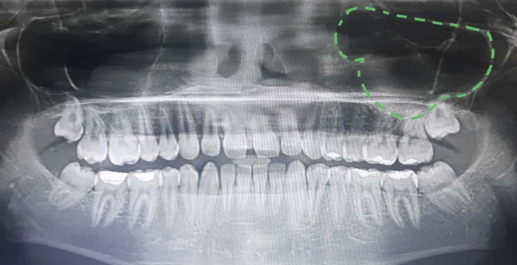
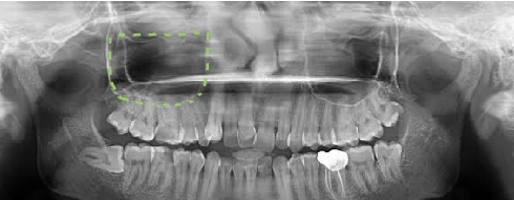
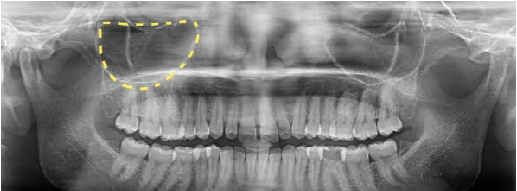
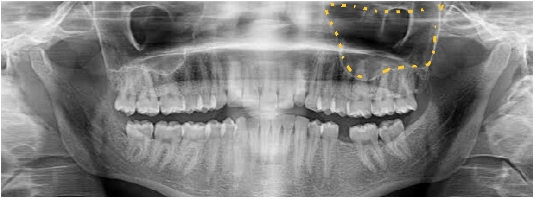
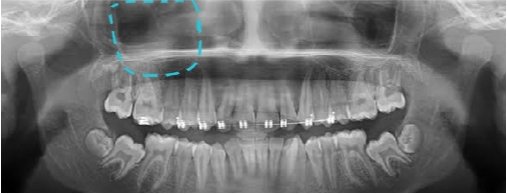
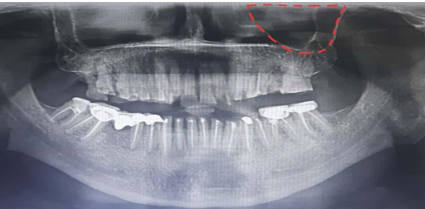
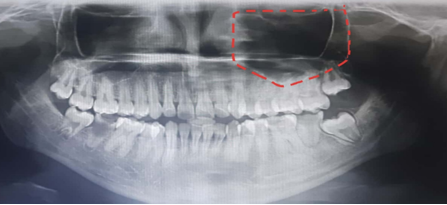
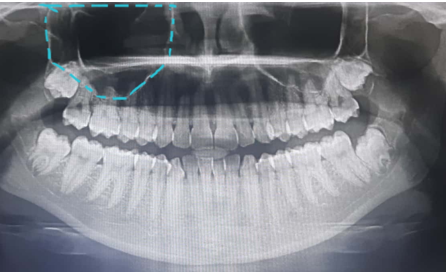
floor and an imaginary line connecting superior points of medial and posterior wall. The shapes includes cloudy, rectangle, round, trapezoidal, square, ovoid, pentagonal, hexagonal. Of which 37% were cloudy ([Figure 5]), 19.5% were found to be rectangle ([Figure 6]). 16.6% constituted round shape([Figure 7]), 13.5% were trapezoidal ([Figure 8]), 7.4% were squarish ([Figure 9]), 3% were ovoid ([Figure 10]) 2.7% were pentagonal ([Figure 11]) and hexagonal ([Figure 12]) which was 0.3% marked the least. The shape predominantly observed was cloudy with rectangle being the second highest. ([Figure 1] Shows pie diagram of classification of maxillary antrum by shape).
Classification by floor
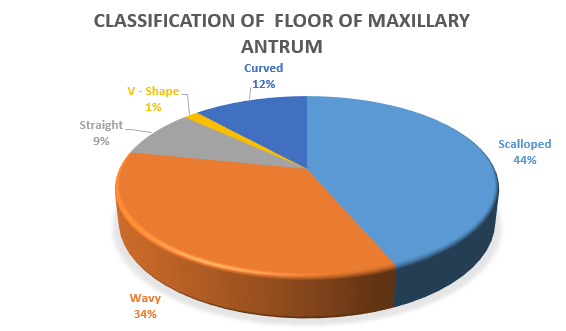
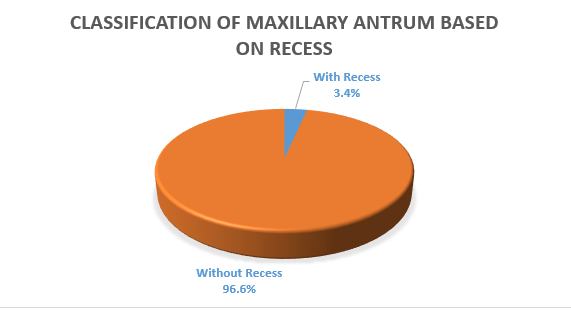
The maxillary antrum we observed showed 6 types of floor contours which comprised Type A-scalloped, Type B- wavy, Type C- curved, Type D- straight, Type E- V shape. In which 43.6% were scalloped, 34.6% were wavy, 11.7% were curved, 8.6% were straight, 1.5 % were V shape. ([Figure 2]. Shows pie diagram of classification of floor of maxillary antrum). Scalloped type found to be the most common and V shape was the least. V shaped sinus floor contour was mostly found in relation to pentagonal shaped sinuses. A few of them showed recess (3.4%) and rest of them were without recess.([Figure 3]. Shows pie diagram of classification of maxillary antrum based on recess).
Classification by septa
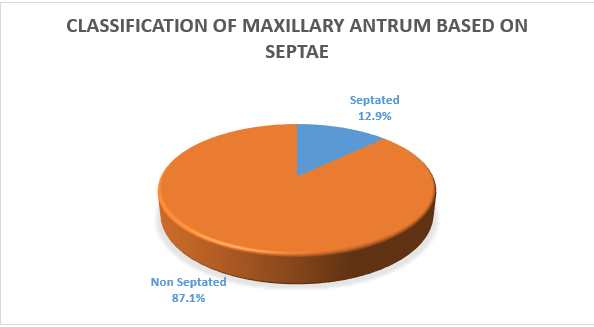
A few of maxillary antrum showed septations(12.9%) , but most of them were without septa(87.1%). Majority of septations were associated with cloudy type(7.7%) and least were associated with squarish(0.6%). ([Figure 4] Shows pie diagram of classification of maxillary antrum based on septae)
Other findings
Among 1000 panoramic radiographs, 358 radiographs showed dimorphism(35.8%) i.e right and left sinuses with different morphology and 658 were similar(64.2%).
Larger right maxillary antrum were noted in 190 radiographs(18.5%). 500 showed larger left antrum (50%) and rest with same size(31.5%).
Discussion
Myriads of findings from several studies portrays the variability of maxillary sinus among individuals. In this study 8 distinct shapes were identified which encompasses cloudy, rectangle, round, trapezoidal, square, ovoid, pentagonal, hexagonal marked the least. Of which 37% were cloudy, 19.5% were found to be rectangular, 16.6% constituted round shape, 13.5% were trapezoidal, 7.4% were squarish, 3% were ovoid, 2.7% were pentagonal and hexagonal were the least with 3%. The predominant shape was found to be cloudy. Similar studies conducted by Aliu A et al with axial CT scan reported five distinct shapes, on the basis of their resemblance to known solids, that included irregular(0.77%), oval(1.15%), quadrangular (1.15%), spherical(23.46%), triangular(73.46) with commonest shape being triangular.[21]
A few of maxillary antrum showed septations(12.9%), but most of them were without septa(87.1%). Majority of septations were associated with cloudy type(7.7%) and least with regard to squarish(0.6%). Howevever, our results were higher than the study by Onwuchekwa et al which showed septation in 7% patients.[22] Comparatively greater percentage(24.62%) of maxillary antrum with septa septa was found by Aliu Abdulhameed et al in CT scan analysis with 1.15 % doubled septa.[23] In cadaveric models, maxillary sinus with septa was found among Canadians, Donal[24] reported a prevalence of 50%, Gabriele[8] among Italians reported a prevalence of 40%, Ella[25] in France reported 38.6% prevalence Maryam[26] in Leuven, Belgium, showed a prevalence 47%. The report of Velasquez- Plata[27] from University of Detroit, Michigan, USA revealed a prevalence of 24% and Won-Jin[28] among Koreans in Jeonju showed a prevalence of 24.6% on CT scan analysis.
In the present study, the maxillary antrums we observed showed 6 types of floor contours which comprised scalloped(43.6%), wavy(34.6%), curved(11.7%), straight(8.6%), V shape(1.5%). Scalloped type found to be the most common and V shape was the least. In another study, Niu et al classified sinus floor contour into Type A narrow tapered, Type B tapering, Type C ovoid, Type D square, Type E irregular. They recommended modified lateral sinus wall elevation (MLSFE) for Type A, both LSFE and Transcrestal sinus floor elevation (TSFE) for Type B and Type C, LSFE with wider for Type D, LSFE with wider window or double window for Type E.[16] In our study, only 3.4% showed recess and rest of them were without recess. Similar to our study Niu et al observed 92℅ maxillary sinus without recess in CT Scan analysis.[16]
Among 1000 panoramic radiographs, 358 radiographs showed dimorphism(35.8%) i.e right and left sinuses with different morphology and 658 were similar(64.2%). Study conducted by Aliu et al.[21] among North western Nigerians reported 85.38% symmetrical sinus which is greater than our finding. In this study, larger right maxillary antrum were perceived in 190 radiographs, 500 showed. Also similar findings were observed by Maryam.[16] However Amusa et al.[29] reported 100% sinus asymmetry, in 24 dried human skulls from southwestern Nigeria, which was found to be comparable with our results. Larger right maxillary antrum in 190 radiographs(18.5%). 500 showed larger left antrum (50%)and rest with same size(31.5%). Similar to this finding Szilvassy observed left antrum to be larger in majority of the CT scan analysed.
Conclusion
This study is a proposed new classification of maxillary antrum using Panoramic radiograph. Panoramic radiograph is the easily available and feasible technology than CT scan. Though it cannot be taken as an alternative due to its limitations, it is supportive and valuable in finding variation especially regarding the sinus floor to some extent. So, like computed tomography it has wide range of surgical, clinical and anthropological significance. From this study, eight distinct shapes of the maxillary sinus were identified, wherein cloudy type was predominant and hexagonal was the least commonest. Only a few had sepatations and recess. Six distinct shapes of floor were identified, of which scalloped marked the highest.
Key Messages
Eight different shapes of maxillary antrum were identified. Among which CLOUDY marked the highest.
Six types of floor observed in which scalloped was predominant and V- shape was the least.
A few of maxillary sinus were septated and with recess.
Almost 35.8% showed dimorphic pairs.
Source of Funding
None.
Conflict of Interest
None.
References
- J T Laitman. Harnessing the hallowed hollows of the head: the mysteriousworld of the paranasal sinuses. Anat Rec 2008. [Google Scholar]
- D LMuszyńska, W Kociemba, A Rewekant, A Sroka, K J Potoczna. Development of the maxillary sinus from birth to age 18. Postnatal growth pattern. Int J Pediatr Otorhinolaryngol 2015. [Google Scholar]
- Y Kawarai. Volume quantification of healthy paranasal cavity by three-dimensional CT imaging. Acta Otolaryngol Suppl 1999. [Google Scholar]
- P Lerno. Identification par le sinus maxillaire. Odontol leg 1983. [Google Scholar]
- J Szilvassy. New Methods about the Intraserial analysis of the excavation areas. Proc Contra Int Symp 1986. [Google Scholar]
- S Maryam, D Xue, Y Hu, J Cleynenbreuge, R Jacobs. Spiral computed tomography based maxillary sinus imaging in relation to tooth loss, implant placement and potential grafting procedure. J Oral Maxillofac Res 2010. [Google Scholar]
- M Malec, T Smektaa, G Trybek, K Sporniak-Tutak. Maxillary sinus septa: prevalence, morphology, diagnostics and implantological implications. Systematic review. Folia Morphol 2014. [Google Scholar]
- G Rosano, S Taschieri, J F Gaudy, D Lesmes, D Fabbro. Maxillary sinus septa: A cadaveric study. J Oral Maxillofac Surg 2010. [Google Scholar]
- A S Underwood. An inquiry into the anatomy and pathology of the maxillary sinus. J Ant Physiol 1910. [Google Scholar]
- H Neivert. Surgical anatomy of the maxillary sinus. Laryngoscope 1930. [Google Scholar]
- G Krenmair, C W Ulm, H Lugmayr. Maxillary sinus septa: Incidence, morphology and clinical implications. J Craniomaxillofac 1997. [Google Scholar]
- N J Betts, M Miloro. Modification of the sinus lift procedure for septa in the maxillary antrum. J Oral Maxillofac Surg 1994. [Google Scholar]
- C W Ulm, P Solar, G Krennmair, G Watzek. Incidence and suggested surgical management of septa in sinus lift procedures. Int J Oral Maxillofac Implants 1995. [Google Scholar]
- L M Ferrin, S G Gil, M R Seeano, M P Diago, D P Oltra. Maxillary sinus septa: A systematic review. Med Oral Patol Oral Cir Bucal 2009. [Google Scholar]
- M Malec, T Smektaa, M Tutak, G Trybek, K Sporniak-Tutak. Maxillary sinus septa prevalence and morphology-computed tomography based analysis. Int J Morphol 2015. [Google Scholar]
- L Niu, J Wang, H Yu. Lixin Qiu New classification of maxillary sinus contour and it's relation to sinus floor elevation surgery. Clin Implant Dent Relat Res 2018. [Google Scholar]
- S C Cho, S S Wallace, S J Froum, D P Tarnow. Influence of anatomy on Schneiderian membrane perforations during sinus elevation surgery: three-dimensional analysis. Pract Proced Aesthet Dent 2001. [Google Scholar]
- G R Velloso, G M Vidigal, D Freitas, O F Manso, G De Brito. Tridimensional analysis of maxillary sinus anatomy related to sinus lift procedure. Implant Dent 2006. [Google Scholar]
- H L Chan, A Monje, F Suarez, E Benavides, H L Wang. Palatonasal recess on medial wall of the maxillary sinus and clinical implications for sinus augmentation via lateral window approach. J Periodontol 2013. [Google Scholar]
- E Bozhikova, N Uzunov. Effects of maxillary sinus floor elevation surgery on maxillary sinus physiology. Eur J Oral Sci 2003. [Google Scholar]
- A Aliu, M S Mohammad, B S Sirajo, A M Abrahim, Z D Abdullahi. Classification of anatomical variants of maxillary sinus shapes and symmetry using computerized topographic imaging. Sub-Saharan Afr. J Med 2019. [Google Scholar]
- N R C Onwuchekwa. Computed tomography anatomy of the paranassal sinuses and anatomical variants of clinical relevants in Nigerian adults. Throatand allied Sci 2017. [Google Scholar]
- A H Dauduza, M S Mohammad, B Abubakar, B S Shiitu, U J Danjuma, A Aziz. Normal anatomical variation of maxillary sinus septa using computarized tomography from Sokoto North western Nigeria. West Afr J Radiol 2016. [Google Scholar]
- D Mcdonnell, M Esposito, M E Todd. A teaching model to illustrate the variation in size and shape of the maxillary sinus. J Anat 1992. [Google Scholar]
- B Ella, N Rda, C Lauverjat, Y Sedarat, C Zwetyenga, N Siberchicot. Septa within the sinus: Effect on elevation of the sinus floor. Br J Oral MaxilloFac Surg 2008. [Google Scholar]
- M Shahbazian, D Xue, Y Hu, J Van Cleynenbreuge, R Jacobs. Spiral computed tomography based maxillary sinus imaging in relation to tooth loss, implant placement and potential grafting procedure. J Oral Maxillofac Res 2010. [Google Scholar]
- D Velasquez-Plata, L R Hovey, C C Peach, M E Alder. Maxillary sinus septa: A 3 dimensional computerized tomographic scan analysis. Int J Oral Maxillofac Imp 2002. [Google Scholar]
- W J Lee, S J Lee, H S Kim. Analysis of location and prevalence of maxillary sinus septa. J Periodont Implant Sci 2010. [Google Scholar]
- Y B Amusa, J Eziyi, O Akinlade, O C Famurewa, S A Adewole, P U Nwoha. Volumetric measurements and anatomical variants of paranasal sinuses of Africans (Nigerians) using dry crania. Int J Med Sci 2011. [Google Scholar]